Why Your VO₂ Max May Be Your Most Important Vital Sign
Cardiorespiratory fitness (CRF), measured precisely by VO₂ max through cardiopulmonary exercise testing (CPET) on the treadmill or bike, is one of the strongest modifiable predictors of how long and how well we live, with risk gradients that exceed smoking, diabetes, and coronary artery disease. It should be a central pillar of any longevity-focused plan, both for day-to-day vitality and for resilience to surgery and serious illness.
What Is a CPET and What Does It Measure?
A cardiopulmonary exercise test (CPET) measures how your heart, lungs, blood, and muscles work together while you exercise, usually on a treadmill or cycle with a breathing mask. The key output is VO₂ max (maximal oxygen uptake), along with thresholds such as anaerobic or ventilatory threshold (AT or VT1) and respiratory compensation point (VT2), which define your personal training zones. Because CPET systems like the one we have at Paradigm measure breath by breath gas exchange, it gives a direct, objective picture of your true exercise capacity rather than an estimate from speed, distance, or heart rate alone which are the metrics used by wearables (e.g. Apple Watch, Garmin, etc).
VO₂ Max, Training Zones, and What CPET Reveals
From CPET, we derive:
VO₂ max: Peak oxygen use (mL/kg/min), a ceiling on your aerobic capacity.
Anaerobic threshold (AT/VT1): The point where lactate and ventilation start to rise; the top of Zone 2.
Respiratory compensation point (VT2): A higher inflection where acidosis accelerates; marks transition into heavy/very heavy domains (Zones 4–5).
This allows:
Precise Zone 2 prescription anchored to your actual AT, not formulas.
Individualized targets to raise VO₂ max (work above VT1/VT2) and improve metabolic flexibility.pmc.ncbi.nlm.nih+1
For a longevity oriented practice, CPET turns “exercise more” into a quantified, titratable intervention and prescription.
VO₂ Max / Exercise Capacity and Longevity
JAMA Network Open “landmark” study
The 2018 JAMA Network Open cohort (Cleveland Clinic, 122,007 patients undergoing treadmill testing) is often cited as the clearest demonstration that CRF is a dominant predictor of survival. The follow-up period was 10 years in this study.
Key points:
All cause mortality fell stepwise as fitness increased and there was no upper ceiling to the benefit achieved.
Compared with “elite” performers, those with “low” fitness had an adjusted hazard ratio for death of ~5.0 over follow up. That is, 5 times more likely to die in the 10-year follow-up period.
The mortality impact of low CRF was like, or greater than, established risk factors like coronary artery disease, smoking, and diabetes when modeled together.
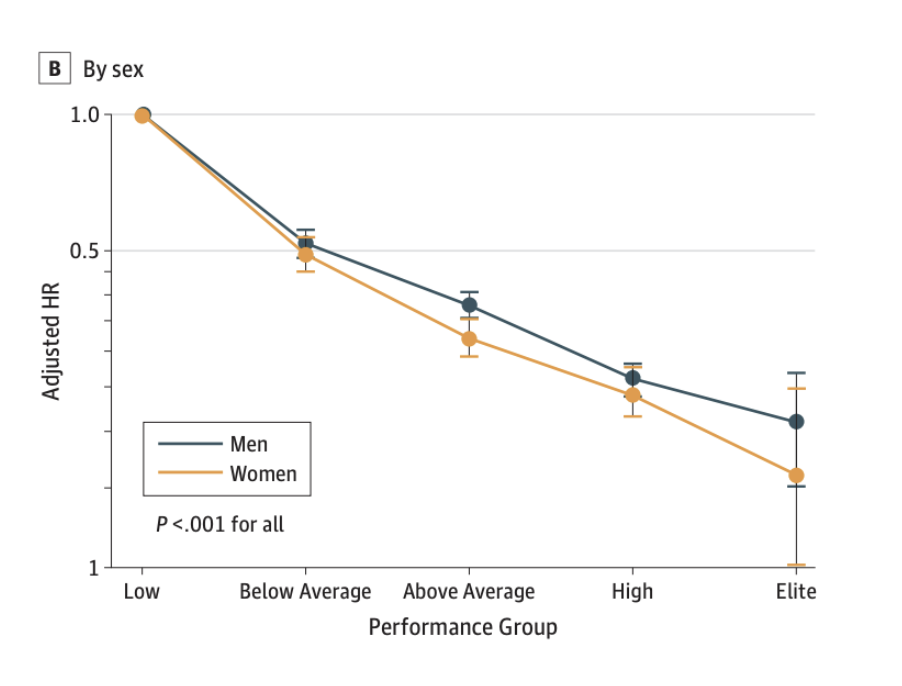
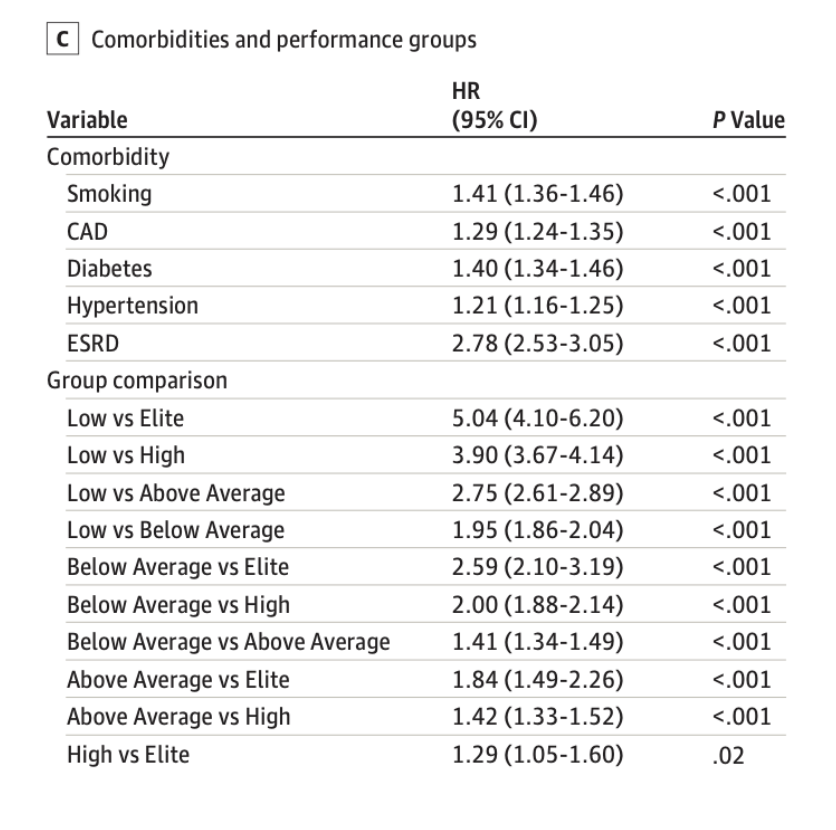
Other large cohorts (e.g., JACC analyses) confirm a graded, inverse relationship between CRF and mortality across age, race, and sex. That is, as CRF goes up, health risk goes down. The figure below shows the association of measured fitness status with risk of mortality. The table shows a comparison of various risk factors as compared to levels of fitness. Of note, the values used in this study were METs (metabolic equivalents) achieved during the exercise test (this is something that we capture on our testing at Paradigm.
VO₂ Max vs Simpler Tests (12-Minute Run, METs)
The JAMA study used treadmill estimated METs (a proxy for VO₂ max) from a standard exercise test, not direct CPET, and still showed extremely strong risk discrimination.
VO₂ max / CPET: Gold standard—direct gas exchange, thresholds, and substrate use.pmc.ncbi.nlm.nih+1
12-minute run / sub-max tests: Cooper style tests and non CPET treadmills can estimate VO₂ max or METs reasonably well and have their own long history linking performance to mortality and CVD events.
For risk stratification and population studies, estimated CRF from simple tests is often “good enough” and clearly predictive. For precision training, perioperative risk, or highstakes clinical decisions such as major surgery, CPET with direct VO₂ measurement and thresholds is superior.
CRF, Cardiovascular Disease, Metabolic Health, and Cancer
Cardiovascular and metabolic disease
Higher CRF is consistently associated with lower rates of:
Coronary artery disease events and CVD mortality, independent of traditional risk factors.
Incident type 2 diabetes and metabolic syndrome, partially mediated through improved insulin sensitivity and body composition.
Each 1MET increase in fitness corresponds to roughly 10–20% lower mortality risk in multiple cohorts.
Cancer
A large Swedish cohort found that higher estimated VO₂ max was associated with lower incidence of colon and lung cancer and lower cancer mortality. Meta analysis suggests high CRF is a strong predictor of decreased cancer mortality overall.
Exercise interventions in cancer patients can improve VO₂ max by several percent, even in the setting of treatment, supporting its use as both a prognostic marker and a therapeutic target.
CRF, Brain Health, and Dementia
Multiple human studies link higher CRF with lower dementia risk and better cognitive performance.
The classic Swedish midlife fitness cohort of 191 women: those with high cardiovascular fitness had an 88% lower risk of dementia (HR ~0.12) and developed dementia ~9–11 years later than medium-fit peers.
A large HUNT cohort analysis showed that sustaining or improving high estimated CRF over time reduced incident dementia and dementia related mortality by ~40–50%, delayed onset by about 2 years, and extended life by 2–3 years vs persistently unfit individuals.
UK Biobank analyses similarly report that higher CRF is associated with better baseline cognition and lower long-term dementia risk, partly offsetting genetic risk.
These are all human cohorts, with doseresponse relationships and biologically plausible mechanisms (endothelial function, cerebral perfusion, insulin sensitivity, inflammation, neurotrophins).
Men vs Women: Any Differences?
Both sexes show strong inverse associations between CRF and mortality, with similar relative risk reductions across fitness levels.
The Swedish midlife cohort suggests women may see especially large relative dementia risk reductions with high fitness, but this is a small, all female sample.
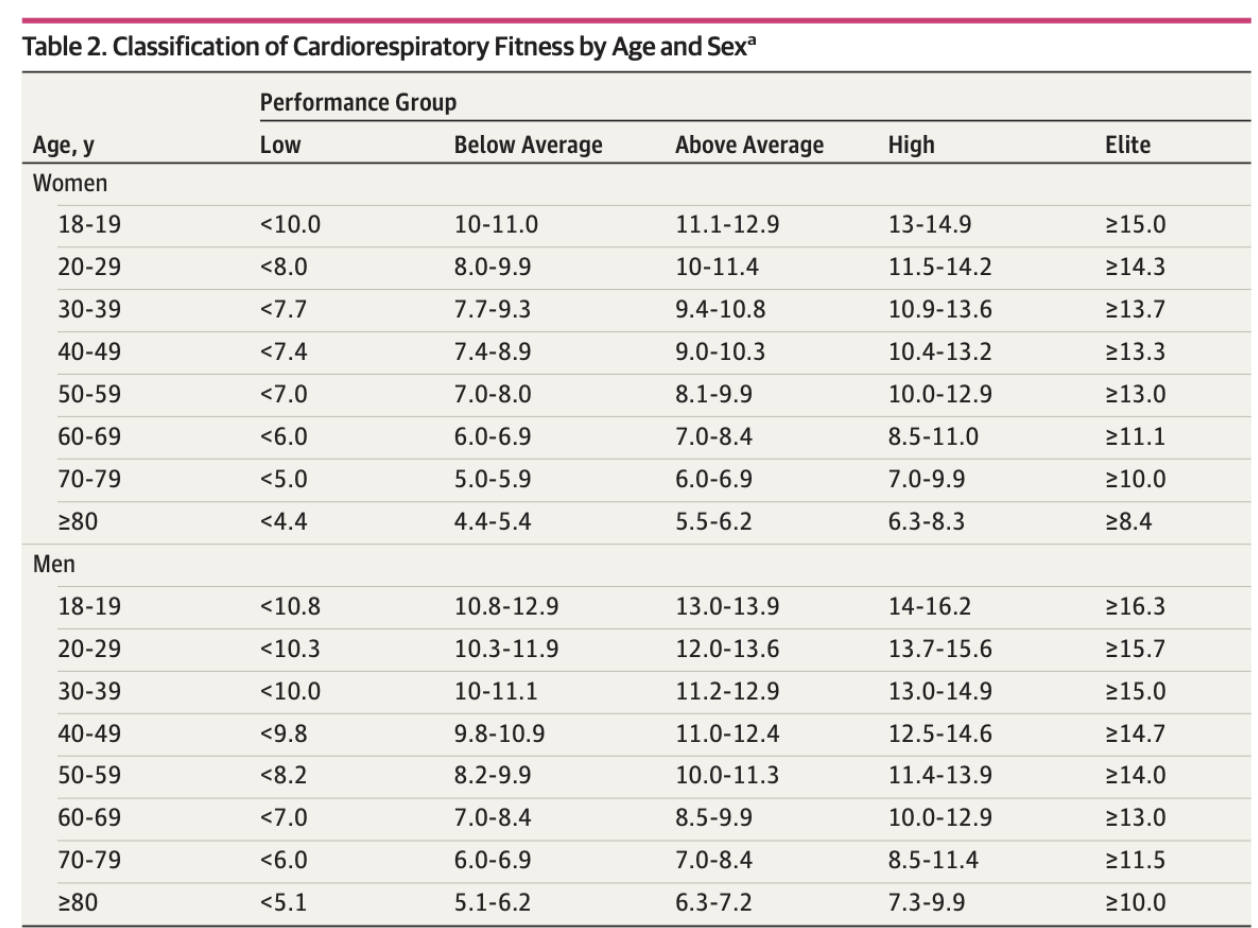
Women often start with lower absolute VO₂ max values (smaller body size, lower hemoglobin, etc.), but relative fitness category (low vs average vs high for age/sex) is what predicts outcomes.
Clinically, the message is symmetric: for both men and women, moving from low to even “below average” CRF yields large risk reductions, and there is no evidence of harm at very high fitness in contemporary cohorts.
Human Evidence: Is Better CRF Really Causal?
The associations are not just cross sectional:
Longitudinal cohorts show that changes in CRF over time track with changes in mortality and dementia risk—those who improve from unfit to fit see large risk reductions vs those who remain unfit.
Randomized training trials in various populations (including cancer patients) increase VO₂ max and are associated with improvements in cardio metabolic risk markers and quality of life, though they are not generally powered for hard outcomes.
While we cannot run lifetime RCTs, the convergence of epidemiology, physiology, and intervention data makes a strong case that improving CRF is causally beneficial.
CPET / VO₂ Max and Perioperative Outcomes
CPET is now widely used to risk stratify patients before major surgery.
Early work (Older et al.) showed markedly higher postoperative cardiopulmonary death when AT/VT1 <11 mL/kg/min.
A recent prospective series in cytoreductive surgery/HIPEC found that patients with higher AT and VO₂ max had fewer complications and shorter hospital stays; an AT threshold somewhat higher than earlier intraabdominal studies was needed given the surgical stress.
Systematic reviews of 30+ studies conclude that CPET variables - particularly AT and VO₂ max - predict postoperative morbidity, need for ICU, and mortality after major abdominal, thoracic, vascular, and transplant surgery.
In practical terms, low CPET performance identifies patients who may benefit from “prehabilitation,” closer monitoring, or altered surgical planning.
CRF and Recovery from Acute Illness
Higher pre-illness CRF is associated with:
Better survival and functional outcomes after cardiac and non cardiac events, including sepsis and respiratory failure, in observational data.
Faster recovery and less functional decline following cancer therapy, where higher VO₂ max both predicts and can be improved with supervised training.
Again, these are human data showing that fitter individuals tolerate physiologic stress more effectively. This is important because it is very important to fully recover from any illness and get back to the pre-illness function level. People with lower CRF have a harder time doing this – and a pattern of losing functional capacity often comes in large steps, such as not fully recovering from surgery, a respiratory illness (e.g. flu), or other acute illness.
How Big Risk Factor Is Low CRF?
The 2018 JAMA cohort allows a useful side by side comparison.
Moving from “elite” to “low” fitness increased 10year mortality risk roughly 5fold.
In the same dataset, conventional risk factors like smoking, coronary artery disease, diabetes, hypertension, and endstage renal disease showed smaller relative risk increments (e.g., CAD ~29%, diabetes ~40%, hypertension ~21%, ESRD ~180%) vs reference.
Put simply, low CRF appears as dangerous – if not way more so - than smoking, diabetes, hypertension, fatty liver, chronic kidney disease, or stable coronary artery disease in many models, and it interacts with them synergistically.
Should VO₂ Max / CRF Be a Core Management Pillar?
Given:
Strong, graded, no ceiling associations with mortality.
Robust links to heart disease, dementia, cancer, metabolic disease, and perioperative outcomes.
Evidence that improving CRF over time improves risk profiles.
It is reasonable to treat VO₂ max/CRF as a primary clinical target alongside blood pressure, lipids, glycemia, and body composition.
Practical Training: How Much in Each Zone?
Literature based prescriptions for raising VO₂ max and CRF in generally healthy adults favor:
Zone 2 (below/around VT1): ~70–80% of training time—easy conversational pace; builds mitochondrial density, fat oxidation, and durability. Think 3-4 sessions per week.
Zones 3–4 (between VT1 and VT2, and just above VT2): ~15–30%—moderate to hard work, including tempo and threshold sessions to push AT and central adaptations. Think 1 session per week.
Zone 5 (well above VT2, very hard intervals): ~5–10%—short, high intensity intervals to stimulate peak stroke volume and VO₂ max. Think 1 session per week or even ending a Zone 2 session with a brief period into Zone 5.
These distributions resemble polarized or pyramidal training models, which are effective for both athletes and motivated adults.
Heart Rate Zones and Orange Theory vs Optimal Training
For simplicity, we can map CPETderived zones onto percent of maximal heart rate (%HRmax) and compare to OrangeTheory Fitness practice, as this is a popular form of cardio.
Heart Rate Zones and Typical / OTF Use
For simplicity, we can map CPET derived zones onto a percent of maximal heart rate (% HRmax) and compare to Orangetheory Fitness practice, as this is a popular form of cardio.
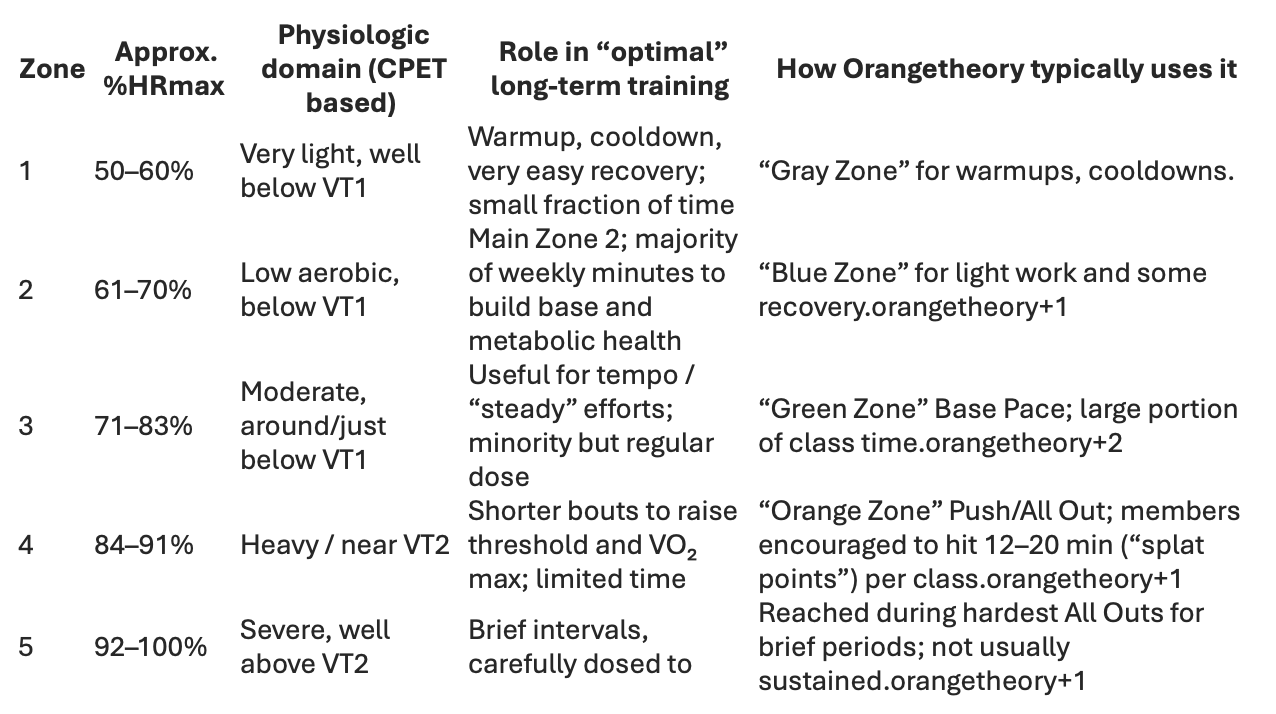
Key differences:
An individualized, longevityoriented plan emphasizes a higher proportion of true Zone 2 (below VT1), which for many people is slightly lower HR than typical OrangeTheory “Green Zone.”
OrangeTheory skews toward higherintensity time (Zones 3–4) in 1hour classes, which is excellent for conditioning and VO₂ max but may underdeliver on lowintensity volume unless supplemented with additional easy sessions outside class.
For your practice, CPETdefined VT1/VT2 can refine these heartrate cut points per patient rather than relying on 220–age formulas. But, it should be noted that any consistent training program is better than none. That is, if you like Orange Theory, then consistently using their system can be of benefit. To truly optimize performance, the team at Paradigm could specify a slightly different plan. But, the main goal overall is optimizing CRF in order topromote your vitality and longevity.